
EMDR for PTSD: How It Works and What the Research Says
Post-Traumatic Stress Disorder (PTSD) is one of the most misunderstood and undertreated mental health conditions. Many people with PTSD don’t recognize their symptoms as trauma-related — they just know that something feels perpetually off: hypervigilant, emotionally numb, easily triggered, unable to trust themselves or others. EMDR therapy has emerged as one of the most effective treatments available for PTSD, backed by decades of rigorous research and endorsed by the world’s leading mental health and medical organizations. Emdr For Ptsd is a topic that comes up often in therapy.
What Is PTSD?
PTSD develops when a traumatic experience overwhelms the brain’s normal coping and processing capacity. Rather than filing the memory as a past event, the brain stores it in a fragmented, dysregulated state — keeping it “alive” in a way that causes ongoing distress.
PTSD symptoms typically fall into four categories:
- Intrusion — Flashbacks, nightmares, intrusive memories of the traumatic event
- Avoidance — Avoiding people, places, situations, or thoughts that serve as reminders
- Negative changes in cognition and mood — Persistent negative beliefs (“I’m broken,” “I can’t trust anyone”), emotional numbing, depression, shame
- Hyperarousal — Hypervigilance, exaggerated startle response, difficulty sleeping, irritability, reckless behavior
PTSD can develop after a single catastrophic event (a car accident, assault, natural disaster) or as a result of prolonged, repeated trauma (childhood abuse, domestic violence, war). Complex PTSD (C-PTSD) refers to the latter — and often involves additional layers of difficulty with emotional regulation, identity, and relationships.
Why EMDR Is So Effective for PTSD
To understand why EMDR works for PTSD, it helps to understand what’s happening in the brain during trauma.
During a traumatic event, the brain’s threat-detection system (the amygdala) goes into overdrive, while the prefrontal cortex — responsible for logical thinking, language, and integration — essentially goes offline. This is an adaptive survival response: in genuine danger, you don’t need to think, you need to react.
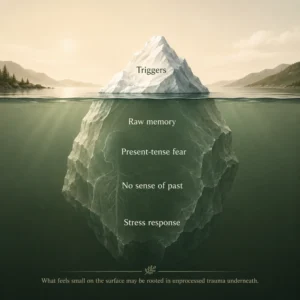
The problem is that traumatic memories encoded in this state — without the integrating influence of the prefrontal cortex — often remain stored in a raw, unprocessed form. They lack the contextual cues that signal “this happened in the past; it’s over; you’re safe now.” Instead, they remain perpetually in present tense, activating the stress response system whenever triggered.
EMDR’s bilateral stimulation appears to engage the brain’s natural adaptive information processing (AIP) system — the same mechanism that processes and integrates daily experiences during sleep. By activating this system while the person holds the traumatic memory in mind, EMDR allows the brain to finally do what it couldn’t do at the time of the trauma: process, integrate, and file the experience as the past.
What Does the Research Say About EMDR for PTSD?
The research on EMDR for PTSD is extensive and compelling:
- Multiple randomized controlled trials show EMDR produces significant reductions in PTSD symptoms
- Studies comparing EMDR to trauma-focused CBT find roughly equivalent outcomes, with EMDR often achieving results in fewer sessions
- Meta-analyses consistently show EMDR outperforms no-treatment and non-trauma-focused treatments for PTSD
- Brain imaging studies show measurable changes in brain activity following EMDR treatment, particularly in areas involved in fear processing and memory integration
- EMDR has been shown effective for veterans with combat-related PTSD, survivors of sexual assault, motor vehicle accident survivors, and those with childhood trauma
These findings led to EMDR being endorsed as a first-line PTSD treatment by the World Health Organization, the American Psychological Association, the Department of Veterans Affairs, and many other major health organizations worldwide. Emdr For Ptsd responds well to focused therapeutic support.
EMDR vs. Prolonged Exposure for PTSD
Prolonged Exposure (PE) is another well-researched trauma treatment that involves repeated, systematic exposure to traumatic memories until the fear response diminishes. Both EMDR and PE are considered evidence-based, first-line PTSD treatments. Emdr For Ptsd is more common than most people realise.
The key differences:
- Amount of verbal processing — PE involves detailed verbal narration of the traumatic event; EMDR requires minimal verbal description
- Homework — PE involves significant between-session homework; EMDR typically involves less
- Mechanism — PE works primarily through habituation and inhibitory learning; EMDR works through adaptive information processing
- Dropout rates — Some research suggests EMDR has lower dropout rates than exposure-based therapies
The best treatment is the one you’ll actually engage with. Many clients prefer EMDR precisely because it doesn’t require extensive verbal retelling of the traumatic event — something that can feel retraumatizing to some survivors. Working through EMDR for PTSD in therapy makes a concrete difference.
What EMDR for PTSD Actually Looks Like
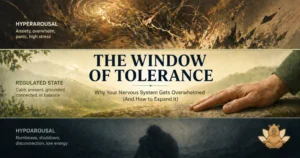
A common misconception is that EMDR involves reliving the trauma in full detail. It doesn’t. EMDR is carefully titrated to keep you within your “window of tolerance” — a zone of manageable emotional activation that allows processing without overwhelm. Emdr For Ptsd responds well to focused clinical support.
In practice, a processing session involves:
- Bringing a specific traumatic memory to mind — the most disturbing image, the associated negative belief, the body sensations
- Following the therapist’s bilateral stimulation (eye movements, taps, or sounds) in brief sets of 20-30 seconds
- Reporting whatever arose during the set — an image, thought, emotion, or body sensation
- The therapist directing further sets based on what emerged
- Continuing until distress reaches a low level and a positive belief feels fully believable
Many clients are surprised that EMDR doesn’t require them to talk through the details of their trauma. The processing happens largely non-verbally, guided by the bilateral stimulation. Some clients process silently; others notice imagery or body sensations shifting without being able to articulate exactly what’s changing. Emdr For Ptsd can be addressed effectively in therapy.
EMDR for Complex PTSD
Complex PTSD (C-PTSD) results from prolonged, repeated trauma — often beginning in childhood. It involves all the symptoms of PTSD plus additional challenges with emotional regulation, identity, self-worth, and relationships. Emdr For Ptsd doesn’t have to stay the same.
EMDR is used for C-PTSD but typically requires a longer preparation phase to build emotional regulation resources before trauma processing begins. For people with C-PTSD, the window of tolerance is often narrower, meaning therapy must proceed more carefully and gradually. Understanding EMDR for PTSD often changes how people relate to themselves.
A skilled EMDR therapist with C-PTSD training will prioritize stability and resource-building before targeting traumatic memories — a principle known as “stabilization first.” Rushing into trauma processing without adequate preparation can be destabilizing and counterproductive. Emdr For Ptsd is more common than most people realise.
How Many EMDR Sessions Does PTSD Require?
Treatment length varies significantly based on the nature and extent of the trauma:
- Single-incident trauma (e.g., car accident, assault): Often 5-12 sessions
- Multiple incidents without a developmental trauma history: Often 12-20 sessions
- Complex/developmental trauma (C-PTSD): Often 20-50+ sessions, with significant time in the preparation phase
These are averages, not guarantees. Your therapist will conduct a thorough assessment and give you a more individualized estimate. Progress is regularly evaluated and the treatment plan adjusted as needed. Working through EMDR for PTSD in therapy makes a concrete difference.
What to Expect When Working on Emdr For Ptsd in Therapy
Many people come in not knowing what to expect from therapy around EMDR for PTSD. The short answer: you won’t be pushed to talk about things before you’re ready, and you won’t be handed a list of affirmations and sent home. Real work on EMDR for PTSD involves building awareness of the patterns — when they show up, what triggers them, what they’re protecting you from — and then slowly building a different response.
The first few sessions are mostly about getting a clear picture of what’s actually going on. Emdr For Ptsd rarely exists in isolation. It usually connects to something deeper — a history, a pattern of relationships, a learned way of coping that made sense at some point and now doesn’t. Therapy creates the space to look at that connection directly.
Progress isn’t always linear. Some weeks things feel clearer; others, something gets stirred up and you leave feeling worse before you feel better. That’s normal. It usually means you’re getting closer to something real. What changes over time is your relationship to EMDR for PTSD — not just your ability to manage it, but your understanding of where it comes from and why it still shows up.
Finding EMDR Therapy for PTSD in Tampa, FL
If you’re in Tampa or the surrounding Florida area and living with PTSD or trauma, Now and Zen Wellness offers specialized EMDR therapy for trauma and PTSD. Douglas Carmody, LCSW, is trained in EMDR and uses a trauma-informed, integrative approach to help clients move beyond survival mode and into a life that feels genuinely livable. Emdr For Ptsd responds well to focused clinical support.
For more on this topic, see the American Psychological Association.
Online EMDR therapy is available for Florida residents who prefer the convenience of telehealth.