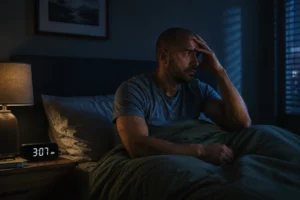
Anxiety and sleep are locked in a cycle that is one of the most frustrating patterns in mental health: anxiety disrupts sleep, and sleep deprivation intensifies anxiety. It’s 3 AM. You’re awake. Your brain is reviewing everything — the conversation that went wrong, the email you haven’t sent, the thing you said five years ago, the thing you need to do tomorrow, whether something is medically wrong, whether your relationship is okay. One thought leads to three. Three lead to twelve. An hour passes.

Anxiety and sleep have a particularly cruel relationship. Anxiety disrupts sleep, and disrupted sleep makes anxiety worse. The cycle feeds itself. And over time, the bed itself — the place that’s supposed to be the refuge — starts to carry its own anxiety charge.This is not insomnia that will resolve on its own. It’s a pattern that needs to be directly addressed. Understanding why it happens is the first step. Knowing what actually works is the second.
Why Anxiety and Sleep Are At War
The nervous system has two modes that are relevant here: the sympathetic (threat response — activating, alert, mobilizing) and the parasympathetic (rest and digest — calming, recovering, restoring). Sleep requires the parasympathetic system to dominate. Anxiety is a sympathetic state. It signals threat. The body responds by increasing cortisol and adrenaline, elevating heart rate, sharpening attention, and scanning the environment for danger.
This is adaptive when there’s an actual threat. At 3 AM in a safe bedroom, it’s just the threat detection system misfiring. Several things make the night particularly fertile ground for this:The protective distraction is gone. During the day, activity — work, conversation, tasks, screens — creates cognitive noise that partially drowns out anxious thought.
At night, the noise stops, and the anxious content moves to the foreground. Cortisol has a natural pre-wake peak. Cortisol, the body’s primary stress hormone, rises naturally in the early morning hours in preparation for waking. People with anxiety disorders or elevated baseline stress often experience this rise earlier and more intensely, which explains why 3 AM is such a consistent wakeup time.
Rumination is a cognitive habit. Lying in the dark with no task to complete, the brain defaults to processing mode — and for anxious brains, that processing often latches onto concerns, plans, and threats. Once the rumination loop starts, it’s self-reinforcing: each thought generates anxiety, which generates more thoughts.
Sleep anxiety compounds the original problem. Many people with chronic sleep disruption develop secondary anxiety specifically about sleep. The worry about not sleeping, about what happens tomorrow if you’re tired, about whether this is going to happen again — that worry itself activates the sympathetic system and prevents sleep. The solution becomes the problem. Working with a therapist who understands anxiety and sleep makes a concrete difference.
7 Proven Ways to Break the Anxiety-Sleep Cycle and Anxiety And Sleep
1. Postpone Worrying to a Designated Time
This is a cognitive technique from CBT that sounds simple and works well. Schedule 15–20 minutes in the late afternoon as your “worry time” — a protected time to review concerns, make notes, and engage with anxious content. When anxious thoughts arise at night, redirect with: I’ll think about this at my scheduled time.This trains the brain to defer rather than suppress. Suppression increases intrusive thoughts. Deferral, paradoxically, reduces them. anxiety and sleep remains one of the most effective conditions to work with in therapy.
2. Practice Progressive Muscle Relaxation or Body Scan
Anxiety lives in the body as well as the mind. Progressive muscle relaxation — systematically tensing and releasing muscle groups — activates the parasympathetic system and gives the body something concrete to do. A body scan meditation similarly shifts attention from thought to physical sensation, interrupting the rumination loop.Neither requires previous meditation experience. Both can be practiced lying down. anxiety and sleep is something therapy can directly address.
3. Get Out of Bed When You Can’t Sleep
This is counterintuitive but supported by strong evidence. Staying in bed while anxious teaches your nervous system to associate the bed with anxiety. Stimulus control — getting up when you can’t sleep, doing something calm in low light until you feel sleepy, returning to bed — preserves the bed as a cue for sleep rather than for wakefulness.This is one of the most effective behavioral interventions for chronic insomnia. anxiety and sleep is far more common than most people realise.
4. Regulate Temperature
Core body temperature drops naturally during sleep onset. Taking a warm shower or bath an hour before bed produces a counterintuitive effect: the subsequent temperature drop triggers drowsiness. Keeping the bedroom cool (65–68°F) supports this process. anxiety and sleep responds well to the right kind of clinical support.
5. Limit Catastrophic Future-Thinking With Scheduling
When the 3 AM thoughts center on tomorrow’s obligations — the meeting, the difficult conversation, the unfinished task — having a written plan (made the night before) that covers the key next steps can interrupt the perceived need to solve these problems right now.The brain ruminates partly because it doesn’t trust that the problem will be handled. Evidence that it will be — a written plan, a calendar entry, a note — can reduce the urgency. anxiety and sleep doesn’t have to be permanent.
6. Reduce Stimulant Use and Screen Exposure Strategically
Caffeine has a half-life of 5–6 hours, meaning that a coffee at 3 PM still has half its concentration at 8 PM. For anxiety-prone individuals, this meaningfully contributes to nighttime arousal. Blue light from screens suppresses melatonin for up to 2 hours. Neither requires complete elimination, but managing both in the 2–3 hours before sleep makes a measurable difference. If you’re exploring help for anxiety and sleep, a free consultation is a good place to start.
7. Address the Underlying Anxiety Directly
This one matters most. Sleep hygiene and behavioral strategies help — they’re real and they work. But they work around the anxiety rather than through it. If the anxiety driving the night wakefulness is chronic and significant, the most durable solution is treating the anxiety itself.
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the gold standard behavioral treatment and has been shown to outperform sleep medication in long-term studies. It addresses the thought patterns, behaviors, and physiological arousal that maintain insomnia. For anxiety and insomnia that co-occur, CBT-I combined with anxiety treatment is the most complete approach. Working with a therapist who understands anxiety and sleep makes a concrete difference.
When to See a Therapist for Anxiety and Sleep
There’s a point where self-management strategies stop being sufficient. Signs that therapy is the right next step:– Sleep disruption has been ongoing for more than a few weeks- Daytime functioning is significantly impaired- You’ve developed anxiety specifically about sleep- The underlying anxiety is affecting other areas of your life (work, relationships, health)- You’re using alcohol or cannabis to sleep — which works short-term and significantly worsens both sleep quality and anxiety over timeTherapy for anxiety in Tampa can address both the sleep disruption and the broader anxiety pattern that’s driving it. EMDR is particularly useful when the anxiety has identifiable experiential roots. CBT directly targets the thought patterns and behavioral cycles that maintain both anxiety and insomnia. anxiety and sleep remains one of the most effective conditions to work with in therapy.
Anxiety Therapy in Tampa and Carrollwood
FAQ
Q: Why does anxiety get worse at night?A: At night, the distractions that partially suppress anxious thoughts during the day are removed, and the brain defaults to processing mode. Cortisol also rises naturally in the early morning hours, which can produce or intensify wakefulness in anxiety-prone individuals. Q: What is the 3 AM anxiety spiral?A: The 3 AM spiral is a cycle where waking triggers anxious thinking, anxious thinking activates the sympathetic nervous system, and that activation prevents return to sleep.
Each thought generates more anxiety, which generates more thoughts. Over time, secondary anxiety about sleep itself joins the original anxiety. Q: Does CBT work for anxiety-related insomnia?A: Yes. CBT for Insomnia (CBT-I) is the most evidence-based behavioral treatment for insomnia and has been shown to outperform sleep medication in long-term studies.
Combined with CBT for anxiety, it addresses both conditions directly. Q: Is alcohol or cannabis okay to use for sleep when anxious?A: Both provide short-term relief and worsen the problem over time. Alcohol fragments sleep architecture and reduces REM sleep, producing less restorative rest. Cannabis disrupts REM sleep and increases anxiety as tolerance builds.
Both make the cycle harder to break. Q: When should I seek therapy for anxiety and sleep problems?A: When disruption has lasted more than a few weeks, is affecting daytime functioning, or involves secondary anxiety about sleep — it’s worth talking to a therapist. The earlier anxiety is addressed, the faster the sleep disruption resolves. For more information, see the NIMH research on anxiety disorders and sleep disruption.
Ready to get support? schedule a free consultation at Now & Zen Wellness in Tampa.